

In previous posts in this deep dive series on wound preparation, we discussed the best needle size and speed of injection for painless anesthesia delivery to an acute wound. In this next post, I’ll examine another thought: why inject at all? Perhaps the use of a topical anesthetic is a better approach.

Many such preparations exist. Traditionally, tetracaine-adrenaline-cocaine has been a choice topical for dermal laceration repair. However, the cocaine part makes many a little uncomfortable. While it’s an effective anesthetic, it’s also an administrative hassle to obtain and safeguard, a high risk diversion drug, and carries a stigma for patients (“You’re going to give my baby cocaine, doctor?”)
Cocaine-containing topical anaesthetics
- AC = Epinephrine-cocaine or adrenaline-cocaine
- C = Cocaine
- MAC = Bupivacaine-epinephrine-cocaine or bupivacaine-adrenaline-cocaine
- TAC = Tetracaine-epinephrine-cocaine or tetracaine adrenaline-cocaine
- TC = Tetracaine-cocaine
A revision of a previous meta-analysis from the Cochrane database, current as of December 2016, concluded that application of a topical anesthetic was an effective, non-invasive method of obtaining anesthesia for superficial laceration repair. This review included 25 RCTs and 3278 patients. They point out that several cocaine-free alternatives exist which provide similar degrees of anesthesia. Here’s a list of some of the commonly used anesthetic mixes and the acronyms by which they are commonly known:
Cocaine-Free Topical Anaesthetics
- Anaesthetic putty (containing 4.94% w/w lidocaine hydrochloride, equivalent to 4% w/w lidocaine base)
- BN = Bupivacaine-norepinephrine
- EMLA = Eutectic mixture of local anaesthetics = lidocaine-prilocaine
- EN = Etidocaine-norepinephrine
- LAT = LET = Lidocaine-epinephrine-tetracaine or lidocaine-adrenaline-tetracaine
- LE = Lidocaine-epinephrine orlidocaine-adrenaline
- MN = Mepivacaine-norepinephrine
- PN = Prilocaine-norepinephrine
- PP = Prilocaine-phenylephrine
- T = Tetracaine
- TE = Tetracaine-epinephrine or tetracaine-adrenaline
- TLP = Tetracaine-lidocaine-phenylephrine
- TP = Tetracaine-phenylephrine
 The authors qualify their results by stating the studies are poor quality, especially when attempts are made to compare topicals vs injectable anesthetic head-to-head.
The authors qualify their results by stating the studies are poor quality, especially when attempts are made to compare topicals vs injectable anesthetic head-to-head.
I say, why compare? It only makes sense to me that (when working in a busy ED or urgent care setting) topical anesthetic should nearly always be applied first when time allows. At best, you’ve saved the patient a painful injection. At worst, you simply follow up with an injected anesthetic, which will probably hurt less thanks to your thoughtful premedication. If nothing else, it gives that patient who is waiting for you to come back after your initial assessment (while you are busy treating a STEMI or a stroke) the sense that you are doing something for them.
Not just for kids anymore
It’s also important to point out that we shouldn’t necessarily reserve topical anesthetics for children alone. A 2017 study showed excellent success at obtaining effective anesthesia in children >8 years old and adults using Lidocaine-adrenaline-tetracaine, with only 23.6% needing additional analgesia.
The strategy was particularly effective when dealing with the subset of wounds that were
- short lacerations (4 cm or less)
- scalp lacerations
- simple finger lacerations
How to do it
If topical analgesia is not already part of your practice, here’s a few things to know from a great, simple primer article. I’ll contrast two of the most commonly used mixtures, LET and EMLA, which are the solutions I use in my clinical practice.
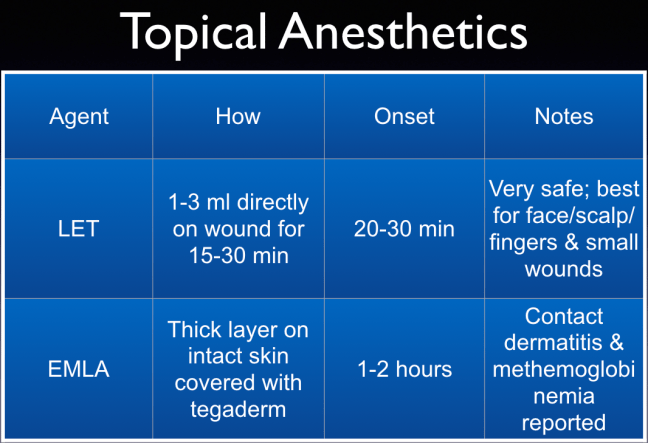
Lidocaine-Epinephrine-Tetracaine (LET)
LET was created as a safer alternative to Tetracaine-Adrenaline-Cocaine. 4% lidocaine simply subs in for the cocaine to create it. It isn’t sold commercially, and will need to be prepared by your pharmacist or nurse prior to use. It can be prepared as a gel (more viscous) or a solution (less viscous). It’s designed for use on non-mucosal skin surfaces including lacerations. You can use a cotton tipped applicator to apply 1-3 ml to the wound with firm pressure for 15-30 minutes. LET is perfect for lacerations as it is absorbed within the wound bed–it actually won’t work on intact skin.
Eutectic Mixture of Local Anesthetics (EMLA)
A eutectic is a mixture of agents that have a lower melting point than any of their constituent parts. At room temperature, the eutectic mixture of lidocaine (25 mg/ml) and prilocaine (25 mg/ml) exists as a liquid and combined with a thickener, emulsifier, and distilled water, allows for a the high concentration of these anesthetics to be delivered in a topical form.
To apply EMLA, spread a thick layer of 1-2 grams per 10 cm2 (maximum dose of 10 grams). Then, apply a patch of tegaderm or plastic wrap which holds it in place. EMLA works on intact skin and directly penetrates the stratum corneum, with a max depth dependent on the total contact time. Application for 60-120 minutes is appropriate; studies show that even after it is wiped off, it continues to penetrate skin layers and provide dermal analgesia for 30-60 minutes.
EMLA is not for use on non-intact sin surfaces and mucosal surfaces. It doesn’t work as well on the palms and soles, where the stratum corneum is thicker and it may not penetrate. Unlikely LET, which has never shown any adverse outcomes in studies, EMLA has a few reported: localized skin blanching, localized erythema, and more seriously methemoglobinemia after prolonged exposure in infants.
Had a good (or bad) experience using topical anesthetics? Any tips/tricks of your own to share? Comment below!
