A 9-year-old boy was brought in for evaluation of facial abrasions after falling down in the schoolyard. He unfortunately fell face first on pavement with loose gravel, causing a painful abrasion around his left eye. The center of the wound was darkened with dirt and debris from the asphalt embedded deeply in the wound, but it was removed with aggressive cleansing using a scrub brush in the ED under procedural sedation. Mom wants to know what happens now–and what she needs to do at home to prevent it from scarring badly.
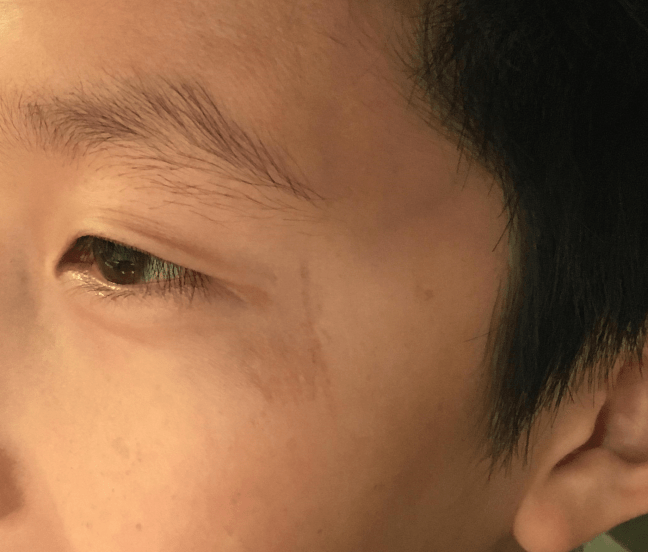
The patient’s facial abrasion, pictured here at 3 months post injury. It’s healing well–what did mom do along the way to get it here? And what needs to be done to ensure it looks even better as time passes?
How would you as a health care provider further manage this wound?
In Part I, we discussed cleansing of dermal abrasions, more commonly referred to as “road rash.” Here in Part II, we’ll discuss how to optimally dress these wounds. If you are a patient and accidentally stumbled on this page, you may want to look here instead: this is an easy-to-follow guide on management of your abrasions after the emergency department or urgent care clinic.
Okay, the wound is clean and debris-free. Now what?
It’s time to package up the patient, and get that wound properly dressed. What’s the optimal method–considering best-evidence, convenience for the provider, simplicity for the patient, and, of course, best long-term cosmesis?
The simplest solution is to apply a layer of vaseline/petroleum jelly covered in a non-adherent dressing. This mimics best evidence-based practice for dressing a laceration after primary closure.
Many patients and health care providers often ask if the use of a topical antibiotic, like bacitracin, confers any additional advantage. While it is tempting to reach for the antimicrobial ointment, keep in mind that this is not an evidence-supported practice, and to the contrary reports exist citing the potentially worse cosmetic outcomes that can result with topical antimicrobials (due to the development of allergic reactions and dermatitis). So, keep it simple: vaseline, non-stick dressing, and an absorbent dressing over this to sop up any exudate. Initially, teach the patient to remove and replace the dressing twice per day, and reduce the frequency as the wound heals/dries out.
But what about all the fancy stuff my office stocks for just this occasion?
Another option that may be available in the office or urgent care setting is the application of any one of a number of commercial dressings. Where I work, there is an entire cabinet stocked with at least a dozen options for dressing wounds, and the sheer number of choices can be dizzying.
To cut to the chase, there is no literature that I am aware of that dictates the optimal dressing for abrasions. If you consider most road rash as more or less equivalent to a superficial partial thickness burn, this becomes easy: there is similarly no single dressing which has emerged as being superior to another for partial thickness burn management. But there are certainly a lot of choices–which makes it confusing.
Not surprisingly, in the context of superficial and deep partial thickness burns, there are a TONof articles comparing different dressings, especially the commercial ones with a lot of financial backing. These sponsored studies show (surprise, surprise) the plethora of advantages for the expensive dressings over cheaper options. Aside from the obvious problem of bias in industry-sponsored studies, this research is very difficult to interpret for myriad reasons. Among them: these studies don’t look at uniform endpoints. Some address pain control, others examine pain with dressing changes, yet others infection rates, others cosmetic outcome or need for surgical intervention. Further, these studies are hard to control, and they are near impossible to blind.
That said, this Cochrane Library review is probably your best go-to for rigorous overviews of the available evidence. The data was collected in 2008, published in 2010, and last updated in 2013. They sought out all RCTs assessing the effects of various burn wound dressings on superficial and partial thickness burns. Thus far they have found 30 (small and methodologically poor) RCTs. They conclude that a number of commercial dressings may have some benefit in the management of superficial and partial thickness burns. These advantage relate to time to wound healing, the number of dressing changes, and pain experienced–but not necessarily to long-term cosmetic outcome.
Ok, I get it, simple dressing vs fancy doesn’t matter. So, how long should dressing changes be continued?
It really depends on what dressing (type) you use. Some absorptive dressings rarely need to be changed, or don’t need to be changed at all (there is your advantage). If you are just using petroleum or bacitracin under non-stick with gauze, you are probably better off changing it daily or twice daily to (1) give the patient an opportunity to look at the wound and inspect for signs of infection and (2) place a new top layer of gauze to handle the messy exudate and (3) make sure that “non-stick” dressing is not actually sticking to the wound–painful!
And what about long-term care for these injuries?
In a line, it boils down to the advice that mama gave you, the same advice that Chicago Tribune columnist Mary Schmich wrote in a 1997 essay, and that Baz Luhrmann famously adapted into a graduation song:
Always wear sunscreen.
To explain the importance of this: sun exposure recruits melanocytes to a wound, ultimately resulting in a darker scar.
I’d also add that there is no evidence to support a lot of the home remedies patients will ask about. Just yesterday someone handed me a crazy cream he bought on a website where the key ingredient was olive oil. While I couldn’t vouch for or against it with great confidence, I definitely could not account for the half dozen additives on the ingredient list. To me, it seemed like an invitation for contact dermatitis and allergy, so I advised skipping it.
Another example is Mederma, which is a gel based on onion extract with claims that it can improve scar appearance. The dermatologists I work with don’t believe in it as studies from the dermatology literature don’t support it. It is probably not likely to cause harm (except to your wallet–$15 for a 20 gram tube!)
Another common one people ask about is vitamin E. Sounds great, theoretically, but this has not borne out well in studies. In fact, some studies suggest a potential detrimental effect in that patients can develop hypersensitivity reactions, urticaria, dermatitis, even erythema multiforme! In fact, in one study there was a suggestion that cosmetic outcome with Vitamin E lotion in the population at large may actually be worse, in part because of these risks. A great reference for this was published in 2006 by Khoosal and Goldman. If a patient insists, make sure they use it on intact skin after the initial wound healing has occurred and that they have proven tolerance to Vitamin E in the past.
If you want to give your patient something a little more accessible, here is a patient friendly version of what a dermatologist at my hospital recommends for aftercare of road rash.
Fortunately, through a combination of meticulous wound care upfront in the ED and attentive care at home after the visit, this patient had a great cosmetic outcome. At three years post injury, normal pigmentation has returned and only a faint hint of a scar remains.
Here’s the same patient from the opening image, revisited 3 years later. While a small scar persists on careful scrutiny, meticulous upfront wound care by the Emergency Physician (and careful attention to the wound by his parents) prevented him from developing a much more unsightly scar.