
Ever come across this problem?
The two situations where I’ve seen it:
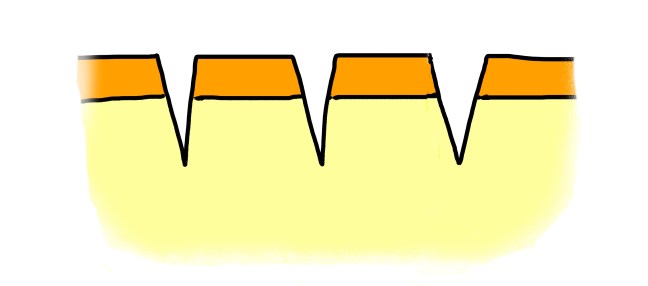
(1) Cutters. The patient with borderline personality disorder, now on a psychiatric hold, who spent the good part of the day prior to arrival making fine lacerations across his/her forearm. Now, in order to be medically cleared for psychiatric hospitalization, you have to take care of the half dozen neatly organized symmetric lacerations…
(2) Jumpers. Specifically, barbed wire fence jumpers. Trying to get free access to the concert, game, etc, this overzealous parkour amateur often ends of with a trail of deep parallel cuts as a badge of honor/shame.
In this post, I share with you the world’s literature on how to handle this problem effectively.
And–spoiler alert–it consists of a back-and-forth conversation in the letters of Annals of EM which occurred in the 1980s. I suppose because it isn’t that frequent of a problem, it hasn’t been re-addressed since then (until now). But some of the concepts discussed in the repair techniques may have wider applications to your daily laceration repair practice…so read on.
The first letter was published in August of 1987 in the Annals of Emergency Medicine. The author suggested the use of a vertical figure-of-8 style suture that crosses through the center flap(s), distributing tension throughout the wound to its healthy margins.
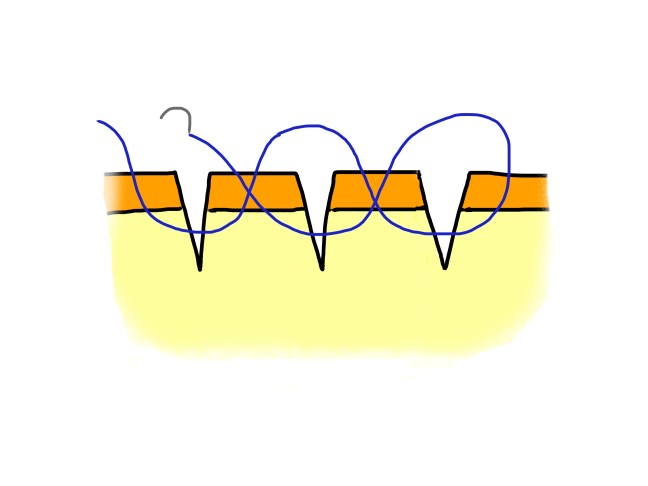
I like this idea, proposed by Dr. Geoffrey Mitchell, if for no other reason than that it is an interesting solution to the problem. It’s versatile and efficient–it can be used in situations with multiple adjacent parallel lacerations. I liked it so much in fact, that it’s featured in this demo video I created below.
A response to Dr. Mitchell’s letter was published in the same journal in March of 1988. Dr. Daniel Samo questioned whether the shape of the figure-of-8 suture would put compressive forces on the edges of the center strip, and potentially cut through the tissue. He alternately proposed placement of a vertical mattress style suture, wider at the base than at the surface, creating eversion of the wound edges on both sides.
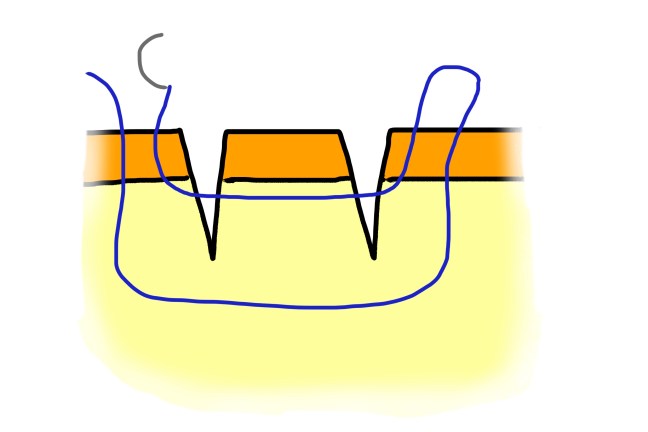
A potential additional advantage of Dr. Samo’s technique is that it can also be used to reattach avulsed islands of tissue.
…which is featured in the demo video below:
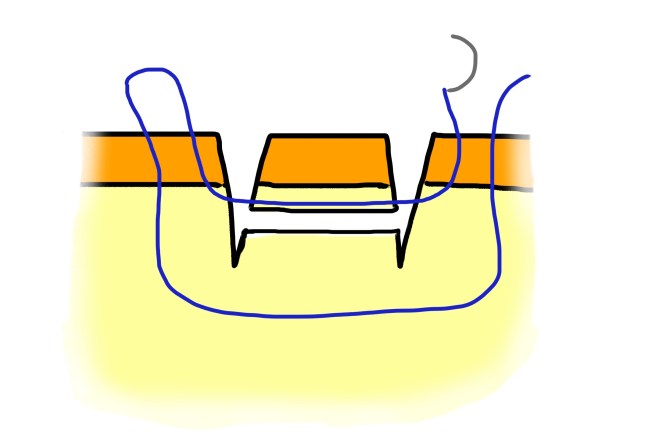
The final thread in this discussion was published in November of 1988 by Dr. Donald Arthur. Dr. Arthur suggested that a horizontal mattress-style suture may actually be the best choice in this situation. He emphasizes that the suture must remain subcuticular through the central flap. He contended that this method had the advantage of approximating the wound edges without distortion, allowing the physician to see how well the edges align.

What’s the ideal method? Hard to say, as again, this was a conversation between experts which occurred 3 decades ago for a problem that just doesn’t seem to occur often enough for us to get too involved in solving it definitively. For my part, I’d say:
- for something rare/novel, a familiar technique is always superior to something you aren’t confident in; thus Dr. Samo or Dr. Arthur’s methods make sense as they draw from familiar patterns like the vertical and horizontal mattress suture.
- for a set of multiple parallel lacerations (3 or more), I might personally consider employing Dr. Mitchell’s technique, which is sure to be a time-saver and properly distribute tension across the multiple strips of tissue.
- we don’t encounter avulsed tissue islands often, and I am guessing there is a tendency to discard that tissue, undermine the existing edges, and close the gaping laceration that is left with a combination of tension-reducing deep dermal sutures and superficial simple interrupted or running percutaneous sutures. But, a back- pocket technique such as Dr. Samo describes for salvaging tissue islands is worthwhile to understand.
