
In a previous post, we discussed needle selection and injection speed as possible influences on a patient’s perceived pain. However, from an evidence-based and statistical standpoint, we ended up with some hand-waving rather than incontrovertible answers.
So if it’s not the needle size nor the time it takes to inject that’s most affecting your patient’s pain experience, maybe it’s more a matter of what you are actually injecting?
In this post we’ll discuss some common practices related to injectable anesthetic use: buffering, use of epinephrine, adding/using bupivicaine, and warming the anesthetic.
Buffering
One customary and well-accepted intervention is to buffer the lidocaine. Lidocaine with epinephrine has a pH=4.0, which is roughly 1000 times more acidic than physiologic pH. Simply stated, you are injecting an acid. Ouch!
Thus, the practice of adding bicarbonate to raise the pH has been advocated as a means to mitigate this pain. A few notes regarding this practice:
- Buffering to reduce pain of injection works on many levels. Aside from less initial pain of injection from a solution at physiologic pH, at pH=7.4 more of the lidocaine molecules are un-ionized and can therefore more rapidly pass through lipophilic cell membranes, which results in a faster time of onset.
- While there are conflicting studies about how well buffering actually works, the preponderance of evidence favors the practice.
- Buffering is generally a just-before-use practice. Lidocaine (especially with epinephrine) stores better in an acidic state. While raising that pH just before use won’t have any effect on efficacy, doing so days in advance theoretically could.
How is it done? Fortunately the recipe to properly buffer lidocaine with epinephrine is pretty simple:
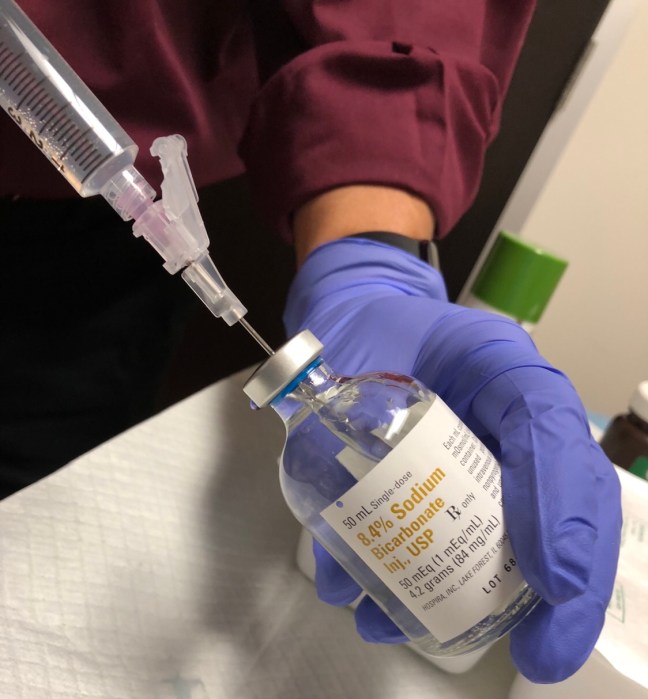
- Using a 10 ml syringe, draw up 1 ml of 8.4% sodium bicarbonate.
- Then, fill the same syringe with 10 ml of lidocaine, for a total volume of 11 ml (yes, the syringe can handle the extra ml), to achieve of a 10:1 ratio that should raise the pH to ~7.4.
- Don’t add more bicarbonate than that. As the pH increases, visible precipitation can occur in the syringe, which can plug the needle and make the solution unusable.
Why is lidocaine with epinephrine better than lidocaine alone?
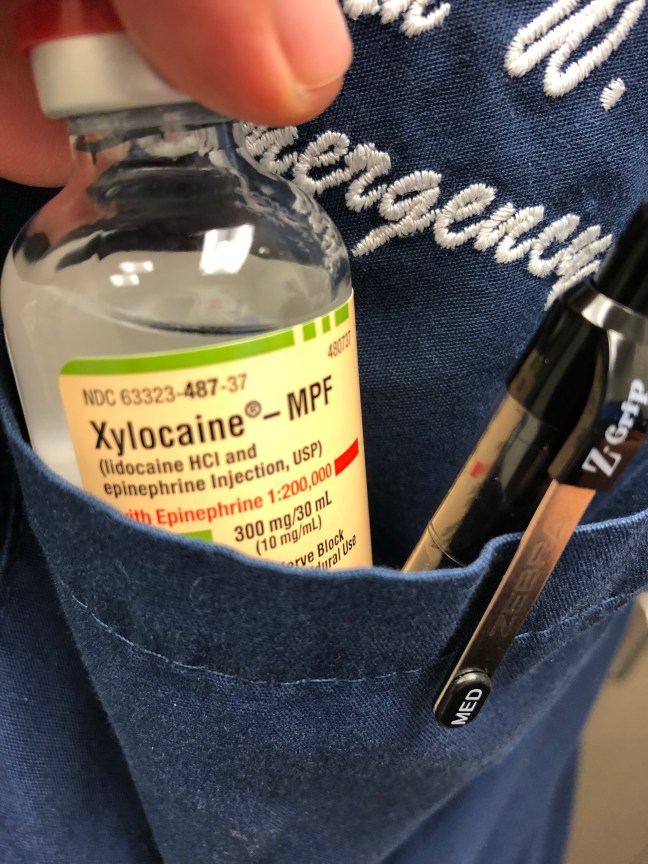
Epinephrine acts rapidly as a local vasoconstrictor, and thus has several advantages. It can reduce bleeding at the site of a fresh wound (facilitating an easier primary closure). It keeps the local anesthetic working locally–therefore a patient can tolerate higher doses without worries of toxicity, and the duration of action is longer since the anesthetic diffuses away more slowly. From a practical standpoint, the operator can visualize the areas already injected more easily, as the lidocaine creates a subdermal blanching effect.
Should I ever avoid lidocaine with epinephrine? Medical dogma dictates that lidocaine with epinephrine shouldn’t be used on the “fingers, nose, penis and toes,” due to concerns about precipitating ischemia from localized arterial vasoconstriction. This myth has been well-dispelled with numerous studies on the fingers (I like this one).
What about bupivicaine?
Some (myself included) prefer to use bupivicaine, an anesthetic with a longer duration of action. It’s certainly a reasonable alternative, and also comes in a preparation with epinephrine. Personally it’s my go-to during a busy shift when I know I will be walking away from the patient and may not get back to him/her for a while. But it isn’t always ideal when you are ready to start your procedure (like cleansing and wound closure) right away, as it may have a slightly slower time to onset.
One recent pilot study explored the idea of getting the best of both worlds, plus buffering. After some work at the bench and trials of use in patients, they proposed that a 10 ml solution of anesthetic should contain:
-
4.5 mL of 2% lidocaine with 1:100,000 epinephrine
-
4.5 mL of 0.5% bupivacaine with 1:200,000 epinephrine and
-
0.4 mL of 8.4% NaHCO3.
This logical combination translated clinically in to an average of 11 hours and 18 minutes of anesthesia per patient, without precipitation of the solution at the bench.
It’s an interesting idea, but it’s probably rare that we need 11 hours of anesthesia for a wound. Also, keep in mind that every additional medicine in a cocktail creates one more opportunity for medication-administration error…
I’ve heard that warming the anesthetic helps with the pain. Is this worth my time?
Another thought is that the temperature of the anesthetic may make a difference. Why might this matter? The thought is that as lidocaine approaches body temperature, it becomes more soluble and thus may have a more rapid onset of action. A meta-analysis of the existing literature published in 2011 does seem to suggest this is true. But like many meta-analyses, it suffers from heterogeneity between studies and many confounders.
This was investigated anew in 2017 by Lundbom, a member of the same group who performed the studies on needle size and speed of delivery.
- This well-designed 2015 Norwegian study used a group of healthy volunteers to compare injection pain using refrigerated 1% lidocaine (~8 degrees C), room temperature lidocaine (~21 degrees C), and lidocaine warmed to near body temperature (~37 degrees C) using a baby food warmer.
- The subjects rated their pain on both a 1-100 visual analog scale and a verbal assessment scale.
- The take-away: heated lidocaine was the statistical winner on both the verbal assessment and visual analog scales, but not by a landslide. In fact, 9 of 36 patients actually reported that they preferred the cold lidocaine to the either room temperature or heated lidocaine.
To me, this speaks to the marked variability in which all humans experience pain.
From a practical standpoint, it’s worth noting that:
- While lidocaine can be refrigerated, it can also safely be stored at room temperature.
- In contrast, lidocaine with epinephrine should be refrigerated.
- Lidocaine in solution can tolerate repeated rewarming.
Summary:
- If you want to be nice to your patient, buffer your lidocaine.
- If you want your patient to be as pain free as possible from start to finish and maybe for another half-day beyond, consider a cocktail of lidocaine-epinephrine-bupivicaine-with buffering.
- Consider warming the solution to body temperature, but don’t lose sleep over it as there’s no guarantee it will make a difference to the patient in front of you.
Next up: why bother with the fuss over injectable anesthetics? We’ll discuss some scenarios where a topical anesthetic may be the right first step.
