
A 30 year old male chef sustains burns of both hands after hot oil spilled on him at work. The wounds are sensate, erythematous, and blanching in all areas. Blistering is beginning to appear, suggesting these are superficial partial thickness burn wounds. Using the rule of palms and confirming with a burn app you estimate a 4% TBSA burn. You arrange urgent follow up with a burn surgeon, as per American Burn Association Referral/Transfer guidelines. You feel he is otherwise stable for outpatient management.
 Superficial partial thickness burns of the palms of both hands, sustained with hot oil while cooking.
Superficial partial thickness burns of the palms of both hands, sustained with hot oil while cooking. Superficial partial thickness burns of the hands, caused by hot oil while cooking. Note the erythema and blistering of the left dorsum of the hand, which was more severely affected.
Superficial partial thickness burns of the hands, caused by hot oil while cooking. Note the erythema and blistering of the left dorsum of the hand, which was more severely affected.Clinical question to be addressed:
How should his wounds be dressed?
While burn wounds begin more or less sterile, these wounds will rapidly become colonized with bacteria. Initially skin flora like Staph epidermidis invade the wound, but then bugs like Pseudomonas, Enterobacter, and E. coli join in the mix. These bacteria can lead to infection of the wound, which is one of the most dangerous causes of burn morbidity. Thus, it’s widely accepted to apply topical antimicrobials to try and keep those colony counts down. There are many types of antimicrobials out there, and many ways to apply them. This blog post will focus on the different options for dressing these wounds. I’ll summarize with a review of the most important evidence regarding use of these dressings, and finally my recommendations.
Silver: Old Faithful
Traditionally, the treatment of outpatient burn wounds involves application of a silver-based solution. It is believed that silver ions inhibit DNA synthesis by bacteria, thus preventing antimicrobial growth.
 Topical silver is the conventional antimicrobial used for burn wound dressings.
Topical silver is the conventional antimicrobial used for burn wound dressings.Silver sulfadiazine (Silvadene) is easy to apply, relatively inexpensive, and readily available; most patients will tell you it actually feels pretty soothing to their wounds.
You can apply it will a tongue blade to a sterile 4×4 to create an occlusive dressing, or apply it directly to the wound surface. Remember, it’s a sulfa-based drug, so you would want to avoid it in a patient with known sulfa allergy.
Sulfamylon is a reasonable alternative for the sulfa-allergic patient. Note that even though the trade name contains the word “sulfa”, mafenide acetate is actually not a sulfa-based medication. Other things to note about this drug– it penetrates an eschar better, but is more painful to apply (to partial thickness burns). As it penetrates deeper, it is usually the recommended antibiotic for burns over cartilaginous areas such as the nose and ears.
Silver nitrate 0.5% solution is another alternative for the sulfa-allergic patient. Chemically it is much like silvadene, but before adding the sulfa-based component. It has overall poorer tissue penetration. It is considered a better choice for Gram negative bacteria and fungal colonization, but this is rarely an issue for the acute burn wound.
Mind you: though silver is a long standing traditional treatment for burn wounds, its use is not strongly evidence supported. A 2014 study suggested that for minor superficial partial thickness burns, applying a layer of petroleum jelly may be just as good. There may even be some evidence that silver is detrimental to some burn wounds. (We’ll get to that.)
Level Up: The Non-Biologic Dressings
Looking beyond silver-based antimicrobials, there is no dearth of products out there that have been specifically produced to treat burn wound injuries. Generally speaking, they can be divided in to: films, foams, composites, sprays, and gels.
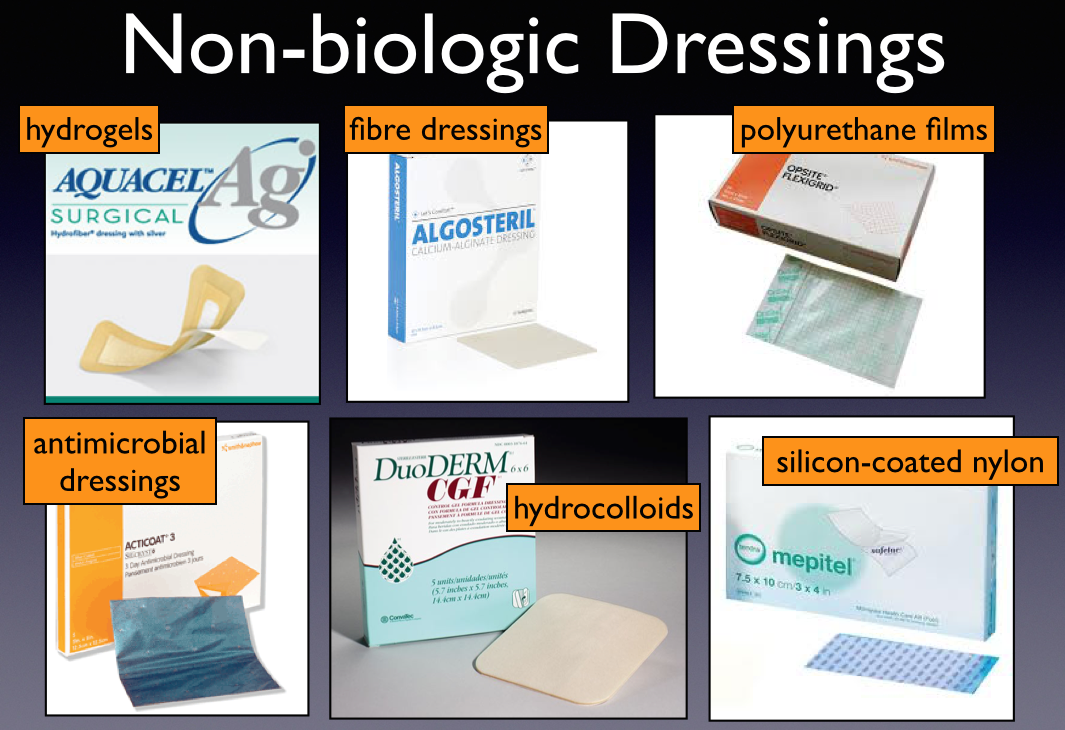 The Non-Biologic Dressings
The Non-Biologic DressingsThe image above is not meant to endorse any product, but just to give you familiarity with some of the products out there. Some of these products combine protective dressings with anti-microbials (generally silver-based, attempting to combine the best of both worlds). Typically the selling points are that these dressings don’t need to be changed as frequently, so they are less traumatizing to the wound. Further, they absorb exudate, thus keeping the wound cleaner and less prone to infection.
Are any of these fancy dressings worth the extra $$$ your department will flow to stock them? …keep reading.
Second Skin: The Biologic Dressings
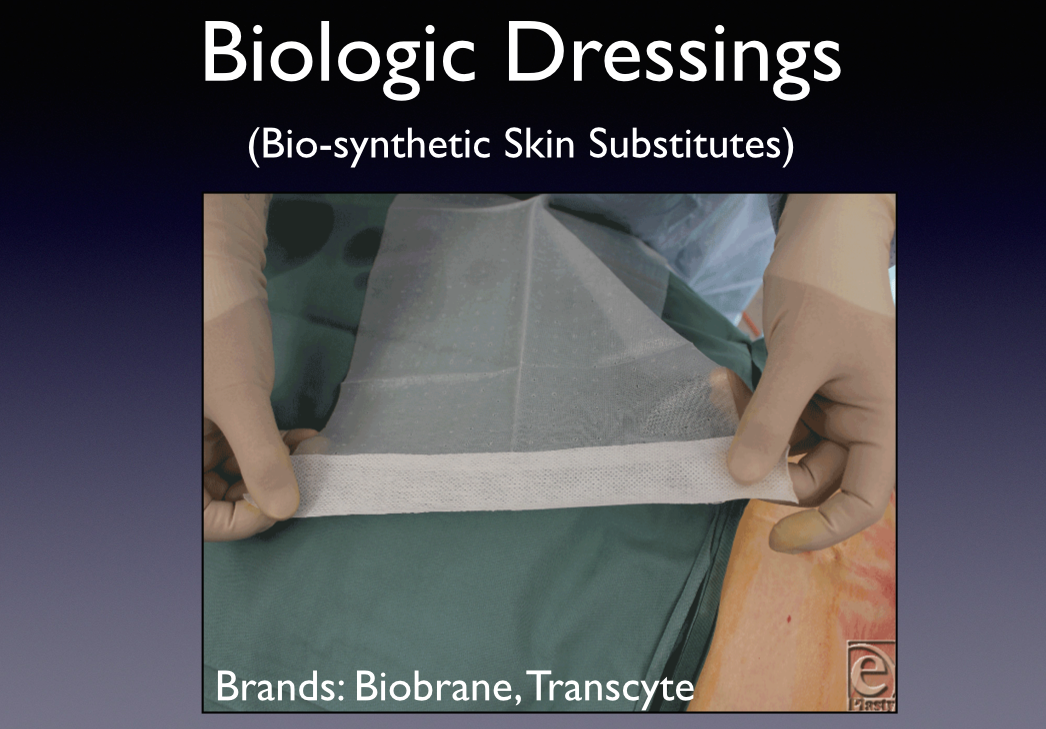 The Biologic Dressings
The Biologic DressingsThe next step up from an anti-microbial dressing is a biologic dressing, also known as a bio-synthetic skin substitute. These fancy dressings use a combination of animal-derived collagen and synthetic nylon mesh to literally act as a “second skin.” The idea behind these dressings is to take on the functions of the lost epidermis until natural re-epithelialization occurs. The material bonds firmly to an adequately prepared wound bed, and spontaneous detaches as re-epithelialization occurs.
One clear advantage of these dressings is ease for the patient. Like the old info-mercials say, you can “Set it, then forget it.” (Not really.) Biologic dressings can be the definitive treatment for superficial and mid-dermal partial thickness burns. Burn surgeons think of it as an alternative worth trying when the patient is on the borderline of needing a skin graft.
The ideal situation for this type of dressing is fresh scald wounds. Typical use is as follows: after applied, it’s kept covered in gauze for 24 hours, and then inspected. Accumulation of pus or exudate under the material indicates need for removal, after which time it would be treated in the standard way with topical antimicrobials. Otherwise, it is left in place until the wound heals.
The success of the dressing as a definitive treatment depends on preparation of the wound bed. The wound has to be very clean to limit infection and exudate which prevents its adherence. Thus, it is best applied in the OR setting, where a patient can get aggressive debridement and cleansing under general anesthesia. However, some burn surgeons do use it in the office setting.
What’s the Evidence?
All of these wound dressing options are pretty overwhelming. So what’s the dressing of choice? To make an informed decision, the first thing you need to know is the price tag on some of these items.
 Costs associated with different burn wound dressings vary widely.
Costs associated with different burn wound dressings vary widely.Application of Aquacel Ag, priced at $108.66 for ten 4×4 sheets, is roughly 7 times as expensive as a single tub of silvadene. With this in mind, you can start to get a little insight in to why this is a hard topic to comment on.
Not surprisingly, there are a TON of articles comparing different dressings, especially the commercial ones with a lot of financial backing. These sponsored studies show–surprise, surprise–the plethora of advantages for the expensive dressings over traditional ones. Aside from the obvious problem of bias in industry-sponsored studies, this research is very difficult to interpret for myriad reasons. Among them: these studies don’t look at uniform endpoints. Some address pain control, others pain with dressing changes, others infection rates, others cosmetic outcome or need for surgical intervention. Further, these studies are hard to control, and they are near impossible to blind.
That said, two systematic reviews are probably your best go-tos for rigorous overviews of the available evidence. The first is a Cochrane library review. The data was collected in 2008, published in 2010, and last updated in 2013. They sought out all RCTs assessing the effects of various burn wound dressings on superficial and partial thickness burns. Thus far they have found 30 RCTs, most of which were small and methodologically poor, limiting the authors’ confidence in their findings. This said, they concluded that a number of commercial dressings may have some benefit in the management of superficial and partial thickness burns. These advantage relate to time to wound healing, the number of dressing changes, and pain experienced. Interestingly, they found that in studies where silvadene was used, there was evidence that it delayed wound healing, and required more frequent dressing changes.
Furthering this data is a second systematic review published in the Journal Burns in 2012. The authors performed an extremely thorough search of the literature for trials comparing topical silver and silver dressings compared with each other, sham dressings, or non-silver dressings. They identified 14 RCTs involving 877 patients. These authors similarly concluded that silver dressings & topical silver are no better, and possibly WORSE than non-silver in preventing wound infection and promoting healing.
Huh?
This data did create a little buzz in the field regarding whether we should be using silver at all to dress burn wounds. You may have heard your local wound care nurse or burn surgeon comment on this.
I have some issues with the conclusions drawn in this study. Truthfully, the odds ratios for the pooled data in these studies were barely significant, and likely not clinically important. But the biggest problem I have is that the studies compare silver to anything and everything “non-silver.” If you look at the studies that they included, this meant anything from Biobrane to topical honey. Bear in mind, topical silvadene is often used as the “control” versus some fancy-schmancy dressing that someone with commercial interests is trying to market, so you have to take it with a grain of salt when they find that the cheaper silvadene dressings are inferior.
The Bottom Line & Final Thoughts
In my opinion, there is insufficient evidence for strong recommendations on the best dressing for partial thickness burn wounds. Routine silver sulfadiazine use is still acceptable, but under scrutiny. We may see recommendations evolving in years to come.
But, not yet. Case in point: I discussed the young man with the hand burns with our on call burn surgeon, who recommended dressing the wounds with silvadene, elevating the limbs, & early range of motion until the patient’s follow up visit.
 The patient in the clinical scenario discussed above had silvadene applied to his wounds. The final dressing involved covering the wound in xeroform and wrapping it loosely with a dry dressing.
The patient in the clinical scenario discussed above had silvadene applied to his wounds. The final dressing involved covering the wound in xeroform and wrapping it loosely with a dry dressing.Don’t get me wrong–even though the evidence for fancy dressings is not strong, I do believe there is a role for more elegant dressing choices in some cases. It may be worthwhile to stock one or two varieties of the non-biologic dressings, for special cases.
 A 14-month-old male with pull-over scald burns from boiling water.
A 14-month-old male with pull-over scald burns from boiling water.For example, take this kid: a 14-month-old with accidental pull-over scald wounds. Imagine the torture you would be putting this kid through if he had to endure twice daily, or even daily dressing changes. He was seen in our ED. We transferred him to a burn center, where he had Biobrane placed and never had to have another dressing change after. I would argue that in this case, regardless of effects on wound healing, there was intangible benefit to the use of a “fancy” dressing.
In the next installment, I’ll discuss the management of a more serious burn wound–one that requires escharotomy.
