
I recently received an email from a practicing emergency physician posing the question:
“I’ve been charged with revamping our suture supplies in a small critical access hospital. I’m a bit ashamed to be somewhat clueless as to needle types. I’ve always just viewed then in terms of “small versus big,” eyeballing them for the appropriate size. Never mind trying to understand the purposes behind different shapes of needles.
Now, however, I feel I should better understand these various options and aspects of suture material before I go ordering a bunch of potentially unneccessary or even incorrect needle shapes. Basically I’m looking for the best, most versatile materials and needle types, without mistakenly ordering seldom used types.
I do appreciate any help or advice you can provide. Thanks again for a great teaching site.”
Kyle Stevens, DO, FACEP
Medical Director, Emergency Department
Molokai General Hospital
Thanks Dr. Stevens! Many great questions packed in to this email. In this two-part post, I will first discuss needles and suture types in general. In part two, I will discuss some considerations in stocking for your clinical setting; teach you how to read your suture packaging; and, summarize what I think is the ideal suture cart for the average ER or Urgent Care treating traumatic skin lacerations.
Understanding Needles
For skin suturing, cutting or reverse cutting needles are the needle shape of choice. These needles are ideal for penetrating tough skin tissue (as opposed to taper point needles, typically used in surgical settings for bowel or blood vessel ligature). Cutting needles are triangular in cross section, with the sharp cutting edge on the inside of the needle curve. These needles are more effective than taper points at piercing the skin surface and smoothly cutting through the dermal layer.
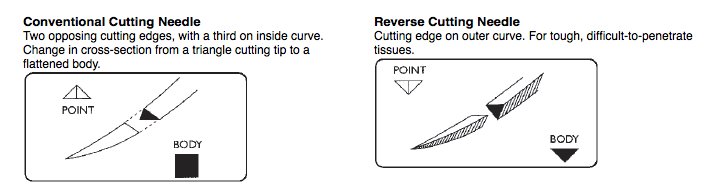 The two major needle types most commonly used in repair of traumatic lacerations. From the Ethicon online catalog.
The two major needle types most commonly used in repair of traumatic lacerations. From the Ethicon online catalog.Reverse cutting needles are similar, except that the cutting edge surface is on the outside of the C-shaped curve of the needle. The idea is to decrease the risk of the suture pulling through the tissue due to the groove in the skin layers that you would naturally form with a cutting needle.
I’ve not found any data to overwhelmingly support the benefit of reverse cutting needles over traditional cutting needles. In my department, we stock cutting needles. Kyle, you are not far off to break it down in to “small” and “large” sizes. Personal preference certainly plays a role here, but three-eights (3/8) of a circle is typically the right curvature for placing a simple interrupted suture in a traumatic laceration. We stock larger 19 mm length needles on our 4-0 sutures for trunk and extremity wounds, and 13 mm length needles on our 5-0 and 6-0 sutures for the finer detail work on the face.
Understanding Sutures
An excellent guide to understanding the different suture materials commonly available in the ED was recently published on the website BoringEM (reviewed by yours truly). This review is geared towards new learners, but is great for anyone looking to review common suture types, and prefaces my recommendations on suture stocking. The following table comes from that post:
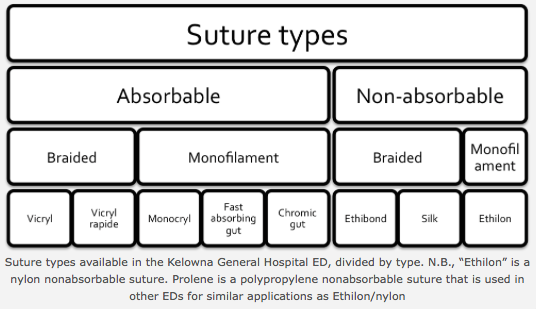 A breakdown of suture types commonly used in the ED. Table initially published at the website BoringEM.
A breakdown of suture types commonly used in the ED. Table initially published at the website BoringEM.The take home point from this table is that sutures really break down in to two flavors: absorbable and non-absorbable. Non-absorbable sutures have traditionally been the suture of choice for most urgent care applications. However, there is an expanding role for the use of absorbable sutures in superficial wound closure.
Sutures can further be subcategorized, as in the above table, based on whether they are mono-filament or multifilament. Another way to subcategorize them is based on whether they are organic or synthetic, but this division is not as clinically important.
The average physician in clinical practice is most interested in how these differences in composition (organic vs synthetic, monofilament vs braided, chromium treated, etc) translate in to ease of handing and usability. These properties include:
- Tissue drag: the coefficient of friction of a suture determines how much resistance one feels when pulling it through tissue. This is somewhat inversely related to
- Tie-ability: a smoother suture doesn’t tie and hold knots quite as well
- Package memory: ever pulled a chromic gut suture from its package and noticed it can’t undue the memory of its u-turns from the packaging? then you know what I am talking about.
Here’s the good news: most modern day synthetic sutures (both non-absorbable and absorbable) have been engineered so well that these small differences in usability will be barely perceptible to the everyday clinician. So, I wouldn’t get too caught up in these details–just having a basic understanding of how composition relates to how a suture handles is good enough.
A separate but related property of sutures of course is their strength, and this is related to the size of the suture. We typically use sutures in the ED ranging from 3-0 (0.3 mm diameter) to 6-0 (0.1 mm diameter) in size. Larger sized sutures hold tension better and are more durable than smaller sizes.
With this background on needles and various suture types, you are ready for my recommendations on stocking…
This will follow shortly in Part II of this post. Stay tuned!
