
I recently read a great article in the Annals of Emergency Medicine describing a case series of traumatic lacerations caused by epinephrine auto-injector devices.
As a connossier of interesting and unique lacerations, I felt obliged to read the article. I have to admit I expected these injuries to be trivial, but I was SHOCKED by just how serious some of these lacerations turned out to be. Many of these were large, deep lacerations that required primary repair in the ED.
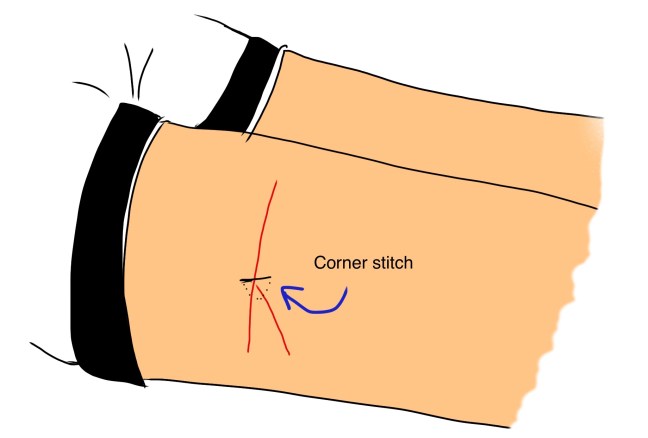
I can’t use the primary source material here for privacy reasons, but here is a cartoon reproduction of one of the lacerations.

It was a long, Y-shaped laceration. It required closure first with a corner stitch,
then each arm of the wound was closed with an unlocked running percutaneous suture.
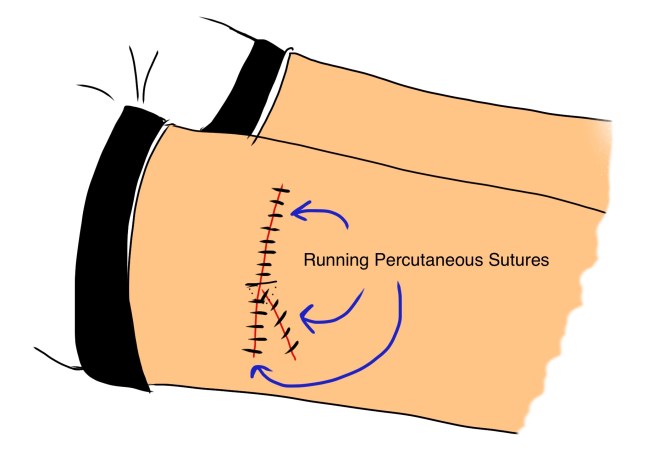
That’s a fair amount of time and effort for an injury that didn’t need to happen!
The lead author of the article, Dr. Julie Brown of Seattle Children’s hospital, gives great summary recommendations for the manufacturers of epinephrine auto-injector devices in her article. Until these become standard issue instructions with the devices, I think a few of her key points are worth sharing with any physician who regularly prescribes Epipen Jr. (or similar devices), to pass on to the parents who may be using them:*
- Immobilize the leg well prior to injection in the thigh. Once the child registers the painful stimulus of the injection, he/she is sure to be screaming, kicking, and fighting–especially if you leave the needle in for the manufacturer-recommended 10 second period. Towards the end of the 10-second mark is when the majority of injuries happen.

- Don’t swing the device like a weapon. One administration technique recommended for use of the Epipen is the “swing and push” method, which requires holding it in the hand like a dagger and swinging it in to the thigh to generate the force to deploy the needle. As it turns out, not needed! The needle is easily deployed with much less force, without the axe-murderer approach (which is likely frightening for children).
- Shorten the insertion time. While the manufacturer recommends a 10 second period of deployment, as Dr. Brown demonstrates in this video, the majority of the medicine is delivered within a second of activating the device:
- Understand the “retracting” needle mechanism. The needle is self-retracting, but only once the device is removed from the soft tissue, causing the spring-loaded needle cover to deploy. If the device is torqued while in use (say, in a fighting child), the needle can bend and the self-retracting mechanism will fail.
- Finally, never re-insert the needle. It may seem silly to us, but some parents/patients/(even doctors!) may believe that the medicine is not fully delivered if that 10-second mark isn’t reached. Not the case, as we discussed above. But worse, trying to re-insert the needle in efforts to make sure the rest of the medicine is delivered is not a good idea. In fact, three of the injuries that were seen were due to a second attempt to get the needle back in.
*NB: Dr. Brown wants to make it explicit that these are her recommendations made to manufacturers. She does not want apprehension regarding use of the Epipen and other epinephrine auto-injector devices to deter parents/patients from using these life-saving devices when indicated.
Dr. Brown’s research was remarkable in the manner in which the data was collected. Rather than using traditional methods of data collection for a clinical study, Dr. Brown and her c0-authors leveraged the power of social media networks to find cases of injuries caused by Epipens and unearth her findings. To learn more about this, see excerpts from my interview with her in Part II, forthcoming.
