
In the next two posts, we’ll discuss the diagnosis and management of vascular injuries associated with traumatic lacerations. In Part I, below, we’ll discuss some of the key points in vascular injury diagnosis. In Part II, we’ll hone in on some specific suturing techniques that can be used to obtain hemostasis when you come across a “pumper.”
To underscore the importance of being prepared to recognize and treat vascular injuries, I’ll open the discussion with this clinical case. This was a real patient I cared for in my ED:
Clinical Case: “It was pumping blood, doc!”
 Laceration overlying the extensor surface of the wrist, caused by a skill saw.
Laceration overlying the extensor surface of the wrist, caused by a skill saw.A 43 year old male walked in to our ED with this laceration caused by a skill saw. An ED triage nurse was the first to assess the patient. The nurse reported that he saw blood “spurting and pumping” from the wound, which led him to apply a pressure dressing and inflate a blood pressure cuff as a tourniquet. It was a busy shift, so it took me a little while to get to the patient. Prepared for the worst, I had an impermeable gown and face mask just in case blood was shooting from the wound as touted. But by the time I evaluated the patient, took the tourniquet down, and removed the dressing…surprise! No bleeding.
What would you do at this point?
I watched the wound for about 15 minutes with no tourniquet, nor dressing, and it remained hemostatic. It was a deep injury, and there were several tendon injuries, which guaranteed a trip at least to the orthopedics OR. But without a pumping arterial bleed, the sense of urgency was lost. The multiple additional ED staff members who had assembled to help me with the patient lost interest and moved on to other tasks.
Nevertheless, I called in a surgery consultation to assess for a possible arterial injury. The triage nurse was a good one, and I trusted his impression. Mine is a teaching community hospital, which means many layers of physicians of different levels of training stand between me and the primary consultant. The surgery junior resident was the first to arrive. He was followed shortly thereafter by the senior resident. Both spoke to the patient and took a cursory look at the wound. Then, deciding that there was no significant bleeding at the time, they declared the vascular injury resolved and signed off on the case.
Still, I wasn’t totally satisfied with this assessment. I called the vascular surgery attending to discuss the case further. Hearing my description of the location & depth of the laceration, he decided to come down and have a look for himself. He took one look at the injury and became livid. He called his residents down to the ER to give them some “teaching.”
He educated the surgical residents that the patient could not be cleared from a vascular perspective until a thorough exploration was performed. This meant anesthesia, irrigation, proper lighting, and a meticulous exam. I thus anesthetized the region, and he performed the exploration. Here’s the result of said exploration:
At the time of this video, he had already ligated one end of the vessel, so the arterial pumping is a little subtle. If you need proof of how impressive it was before the ligation, note the blood that spurted on to the shoulder of his white coat prior to the ligation, seen at the end of the video.
The pearls I learned from this case were:
(1) When someone, anyone, no matter what his/her level of training–nurse, technician, even a layperson–describes blood was “spurting” or “pumping” from a wound, this is an arterial injury until proven otherwise.
It is important to keep this in mind, especially in light of the fact that many of these wounds will be hemostatic by the time you get to assess them. Within hours of the initial injury, vasospasm occurs and small thrombi form at the injury site which can obscure significant arterial injury. This is especially likely if the patient has had some tourniquet time, as this patient had. Pressure and tourniquets slow the flow and allow a more substantial and organized clot to form. Make sure to explore that wound to look for the injury, and call upon qualified personal to assist if needed. Oh, and…remember to wear protective gear.
(2) It pays to review your anatomy before exploration of a wound.
This way, you know what major vessels you are looking for, and what the consequence of ligation of any given vessel would be. For example, in this case the laceration lied transversely over the anatomic snuff box, creating a high risk of a deep radial artery injury. This was exactly what we discovered when exploration of the wound was performed.
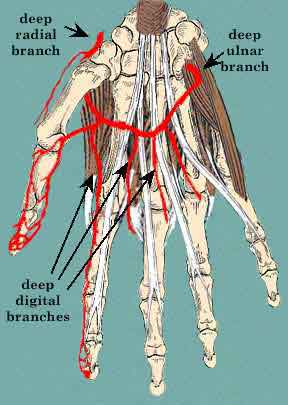 The deep radial artery branches from the radial artery to form the deep palmar arch, supplying blood to the fingers. Figure from http://home.comcast.net/~wnor/lesson5artofhand.htm, by Dr. Wesley Norman.
The deep radial artery branches from the radial artery to form the deep palmar arch, supplying blood to the fingers. Figure from http://home.comcast.net/~wnor/lesson5artofhand.htm, by Dr. Wesley Norman.The standard of care to exclude occult vascular injuries caused by minor lacerations (by this I mean, in the distal extremities, without a major penetrating trauma mechanism like knife or gunshot wound, or hard signs of vascular injury) remains a detailed physical exam. Despite the advent of angiographic imaging techniques, nothing has been proven to beat a careful exploration (for these types of injuries). But, the provision to this is that you need to know what you are looking for in the given anatomic region. If you are not sure that you do…whip out your Netter’s anatomy textbook before you go digging!
(3) Have some techniques in your back pocket to manage an arterial bleed, before you find it.
Bleeding from tiny arterial bleeders and venous “oozers” can often be controlled with direct pressure–in other words, the compression created by just closing the wound in the usual fashion. When that fails, for small bleeders (less than 2 mm diameter) you might also consider use of lidocaine with epinephrine or an electrocautery device. When transection of a more significant arterial vessel (greater than 2 mm diameter) is discovered, options include ligation versus primary repair of the vessel.
In the case discussed above, given the collateral circulation provided by the deep branch of the ulnar artery, ligation of both ends of the transected vessel was a safe option. But it is important to recognize that depending on the location of the injury, this may not always be the best decision. If the patient lacks rich collaterals, or the vessel injury is proximal enough, surgical repair may be indicated. This is why we as emergency providers need our vascular surgeons to weigh in on the majority of these cases.
You may be asking: Why does it matter if you miss a vascular injury in the distal part of an extremity?
Most of the time, these are not life- or limb threatening injuries. Rarely will a patient bleed out from one of these wounds. Generally (except for some digital injuries), adequate collateral circulation exists to prevent infarction of the distal extremity. But there are complications that can occur that you do need to worry about: pseudo-aneurysms, dissections, occlusions, and fistulas in the extremities may not be lethal, but may cause significant disability or deformity. Just last year, in the Annals of Emergency Medicine, an interesting image of a child who developed a pseudo-aneurysm due to an undiagnosed arterial injury within a hand laceration was published. These complications really happen!
It’s important for emergency medicine providers to be facile in at least a few techniques of small vessel ligation, as even a small arterial pumper can lead to some messy and hair-raising situations. In Part II of this post, I’ll discuss a few of the techniques I like to use for vascular ligation–and, show some video footage of putting these techniques to work in a real patient care situation!
