
Clinical Case:
A 45 year old female presents within hours of this scald burn injury to your ED.
 A 44 year old female with a scald burn injury to her trunk and arm.
A 44 year old female with a scald burn injury to her trunk and arm.
Question for consideration:
How deep is this burn, and how do I document it/communicate its severity to a consultant?
Burn wound depth is one of three major factors that essentially need to be determined hand-in-hand when performing an initial assessment. The second is burn wound total body surface area, which we will cover in Part II. Finally, the anatomic location of wounds can lead to special considerations in terms of immediate management and disposition, and we’ll cover this in Part III. This post focuses on burn depth severity grading.
Burn Severity Grading
 Burn Severity Grading
Burn Severity GradingThere are several systems out there for grading burn depth severity.
The traditional system uses a 1st, 2nd, and 3rd degree grading system. This schema was devised in the 16th century by the French surgeon Ambroise Paré and to a degree (pardon pun) remains in use today. A more precise and medically accepted system uses description of the skin layers involved.
Then there is my system, which is really just trying to figure out: who needs a skin graft, and who doesn’t. In truth, this is how most burn surgeons really think about the wounds that are referred to them, as it dictates the urgency of a transfer. This is no small consideration given that Burn Center beds are a scare resource.
Let’s review each type of burn injury, but out-of-order: first, the “easy” ones (1st and 3rd degree); then, the often more confusing 2nd degree burns.
First Degree/Superficial Burns
 A superficial (aka first degree) burn wound injury, sustained on the leg of a patient on an all day river rafting trip without sun protection.
A superficial (aka first degree) burn wound injury, sustained on the leg of a patient on an all day river rafting trip without sun protection.A first degree burn, also known as a superficial burn or epidermal burn, implies only involvement of the epidermis. These burns are sensate (usually extremely painful), blanching, and erythematous. The typical analogy used here is a sunburn. Be weary of using the terms interchangeably, however. While most sunburns are included among first degree burns, they are not the only cause of superficial burns. And vice versa: intense and prolonged sun exposure can certainly cause deeper injury than just a superficial burn.
While superficial burns are quite painful, they are benign in nature. These are expected to heal in 3-5 days without scarring. For this reason, these ARE NOT included in burn wound total body surface area (TBSA) assessment.
Third Degree/Full Thickness Burns
 A full thickness burn wound to the hand of a child. Note the white, waxy areas surrounding erythematous areas of partial thickness burn.
A full thickness burn wound to the hand of a child. Note the white, waxy areas surrounding erythematous areas of partial thickness burn.On the other end of the spectrum, third degree burns, also known as full thickness burns or deep dermal burns, imply complete involvement of the epidermis and dermis. As nerves and vessels are obliterated in full thickness burns, they are painless and non-blanching. Other descriptors are often associated with these burns: white, waxy, or brown coloration (note the variability). The presence of overlying eschar is also characteristic. Since these findings are more variable, your best bet is to test sensation and capillary refill when you suspect this depth of burn. All but the most minor of full thickness burns need to be referred to a surgeon for excision and grafting.
Second Degree/Partial Thickness
 Partial thickness (second degree) burn from a pull-over scald in a young toddler. Would you be able to tell on initial ED evaluation if this patient needs a skin graft? Don’t feel bad if you can’t.
Partial thickness (second degree) burn from a pull-over scald in a young toddler. Would you be able to tell on initial ED evaluation if this patient needs a skin graft? Don’t feel bad if you can’t.These are the majority of the burn wounds that we see in the ED, and thus warrant a more extensive discussion.
These wounds can be tough to call, as their appearance is variable. By definition, the injury involves damage to the dermis, but the appearance and examination varies depending on the exact depth of dermal involvement.
These wounds will all be sensate and painful, though a deep partial thickness burn will be less painful than a superficial one. Both wounds will blanch with pressure, but this may be harder to notice in a deep partial thickness burn.
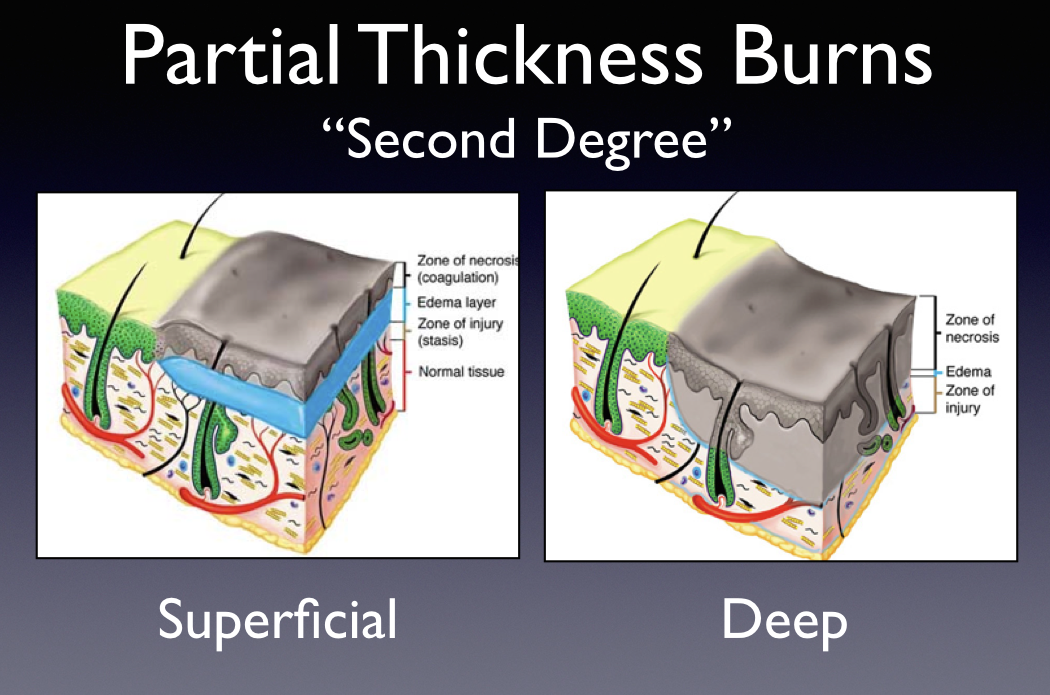 This cartoon depicts the varying pathology described by the term “second degree burn.”
This cartoon depicts the varying pathology described by the term “second degree burn.”Blistering is much more commonly seen in superficial partial thickness burns. This is due to the presence of edema in between the epidermal and dermal layers (shown in blue) in a superficial burn. In a deep burn, the damaged epidermis and dermis are often adherent to each other.
 The myriad appearances in patients described as having “second degree burns.”
The myriad appearances in patients described as having “second degree burns.”A word to the wise: if you are not sure or have any doubt about the exact depth of the wound, state so in your chart, and don’t let a consultant force you to commit. Remember my “bottom line” grading system? When you designate something as “superficial partial thickness,” you are essentially stating that you expect a benign course for the wound. A superficial partial thickness burn is expected to heal with minimal scarring in 10-14 days. In contrast, a deep partial thickness burn will take much longer to heal, will often heal poorly, and have a higher infection risk with worse cosmetic outcomes. Most of these patients will actually require skin grafting.
So–you can see how important it is to differentiate a superficial from a deep partial thickness burn. The reality here is that sometimes, even an experienced burn surgeon can’t tell you what type of wound it is based on initial clinical examination. Another reason why it’s hard to label the thickness of a partial burn wound on initial exam is because in a sense, it may not yet be completely determined. This brings us to an important concept which is…
Burn-in-evolution
The thinking here is that when a burn occurs, there is an innermost layer, the zone of coagulation, which is the part of the burn nearest the heat source–this is the dead tissue that is unsalvageable.
In contrast, the outermost layer of the burn is the zone of hyperemia, where blood vessels are dilated, and capillary leak of plasma and inflammatory mediators occurs. This area is well perfused and has a good prognosis.
Between these is a zone of stasis, where circulation is impaired, but immediate cell death has not occurred. It’s the zone of stasis that has a nebulous fate, which is largely dependent on the resuscitation that the patient receives in the first 24-48 hrs.
 Depiction of the “burn-in-evolution” model.
Depiction of the “burn-in-evolution” model.In summary: I do think there may be some cases where it is perfectly reasonable (and probably safer) to hedge your bet and label these burns as “partial thickness or second degree burn, indeterminate depth” on your initial examination. This is a way of communicating to a burn surgeon that you have a wound on your hands that doesn’t require immediate, emergent action, but you are still worried about it. Depending on the TBSA and other patient characteristics (e.g. social factors, sensitive body areas like face and hands) management of these wounds may involve scheduled follow up exams by a burn specialist on either an inpatient or outpatient basis.
To come full circle, referring back to the clinical case:
This patient had full sensation in all of her burnt skin areas, which is a critical part of the assessment before attempting to grade the injury.
A 44 year old female with a scald burn injury to her trunk and arm.I would describe her wound as a partial thickness burn or second degree burn, indeterminate depth. Blistering in many parts of the wound favors a superficial partial thickness burn, but a mixed superficial and deep partial thickness burn injury cannot be ruled out (on initial examination), especially given the presence of the salmon-colored, desquamated area in the center of the photo.
That sums up Part I. In the next post, we’ll discuss updates in accurate and rapid TBSA assessment, and how this effects treatment/disposition.
