
This final installment is part of a series of posts meant to expand upon and complement a great article that was just published in ALiEM regarding the evaluation and management of extensor tendon injuries. Rather than give redundant information, in these posts, using images and videos, I hope to bring to life some of the specific concepts discussed by Dr. Baylis, Dr. Ting, and Dr. Haythornthwaite.
Issues at play
The goals of an extensor tendon repair are: to maximize strength in order to preserve function and prevent re-injury; to minimize the tendon shortening which is an inevitable consequence of pulling the two ends together; and to reduce the foreign body effect which can cause adhesions and decrease the “glide” of the tendon in the long term.
Given these issues, research in this field focuses on best sutures to use for repair, best techniques to use for tendon repair, and sometimes whether primary repair (as opposed to immobilization) is the best strategy at all. These links will take you to some of the more recent articles/reviews in this field if you are interested, but this post focuses on the nuts and bolts of repair for the everyday Emergency Physician or Urgent Care Practitioner.
Choosing your suture
Though many different acceptable choices exist, your best bet is likely a non-absorbable suture with low tissue reactivity and sufficient strength to hold the tendon without cutting through it. As such, a synthetic suture such as ethibond or mersilene is a good choice. Depending on the size of the tendon at the site of injury, 3-0 or 4-0 would likely be the appropriate size.
Repair Techniques
Suturing through and through the lacerated ends of a tendon to re-approximate the tendon is referred to as core suture placement. This is in contrast to an epitendinous suture, which means suturing through the external sheath of the tendon. The extensor tendon distal to the metacarpal-phalangeal (MCP) joint is relatively flat, and thus amenable to suture techniques familiar to the average emergency physician, such as the horizontal mattress suture or figure-of-eight. The obvious advantage here is that these suture patterns are readily familiar to physicians practicing in multiple specialities who regularly deal with laceration repair.
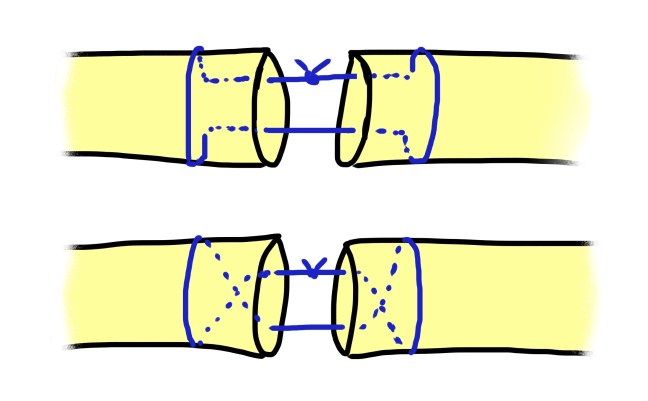
Proximal to the MCP, where the tendon is generally larger and more rounded or semi-circular, one may consider a “grasping” core suture technique. The advantage of this type of suture is that it literally grasps the parallel fibers of the tendon, and is thus less likely to tear through the frayed ends of a damaged tendon. The following video gives a short tutorial on how to perform two common grasping suture techniques.
The grasping suture techniques go by many eponyms: the modified Kessler suture, the modified Bunnell suture are most commonly touted, but this nomenclature can be confusing as different experts will actually describe similar–though not identical–techniques using these terms. Not to minimize the contributions of the many incredible surgeons who worked to develop these techniques, but the importance in clinical practice is to have command of at least one common variation and understand when to employ it.
Take Home Points:
- Understand the goals in suturing a tendon to facilitate better repair.
- A 3-0 or 4-0 synthetic absorbable suture is generally the suture of choice.
- Learn a “grasping” core suturing technique to increase your prowess for repair of complex extensor tendon lacerations.
