
A 19 year old patient (they/them/theirs) was in a rush and slammed their finger in the car door on the way to work. Now, they are making a detour to your ER with this injury:

An X-ray is performed and reveals that this is not just a laceration–this is an open fracture of the distal phalanx. You recognize the immediate danger an open fracture represents for the patient and get on a call with your friendly neighborhood orthopedic surgeon to describe the injury.

Upon hearing the story, she states, “Okay. Sounds like it’s just an open tuft fracture. Wash it out really well, close the laceration, and give them a gram of cefazolin. Send them home with a week of cephalexin and refer them to see me next week.”
Huh. You feel confused and not sure you entirely trust this advice. Isn’t an open fracture an orthopedic emergency? Doesn’t this patient need to go to the OR for a washout? What should you do?
Questions to consider:
- What is a “tuft” fracture?
- Is it ok treat this open fracture so differently than we treat other open fractures?
- How do I splint this thing for the best functional and cosmetic outcome?
- Is giving antibiotics an evidence-based best practice?
- Do these patients need to see an Orthopedic surgeon/specialist in real time, or at least in follow up?
In Part I of this post, I’ll address questions 1-3; in Part II, I’ll answer questions 4-5 AND let you know how this particular case resolved, with a bonus wrap-up video!
A few requisite words on scope of the problem
Phalangeal fractures are the most common injuries in the body. They account for 10% of all fractures and 1.5% of all ED visits. They happen more often in men than women.
Put simply, we see these a lot. When I work minor injury, I probably see one every few shifts! In truth, I’ve managed them like the orthopedic surgeon describes above, but I’ve never put much thought in to the why: historical reasons, treatment rationale, and evidence-based practice to support it.
Anatomy Primer: What exactly do we mean when we call something a tuft fracture?

- Let’s start with some precision. Not every fracture of the distal phalanx is the same, and only a small portion of the distal phalanx comprises the tuft.
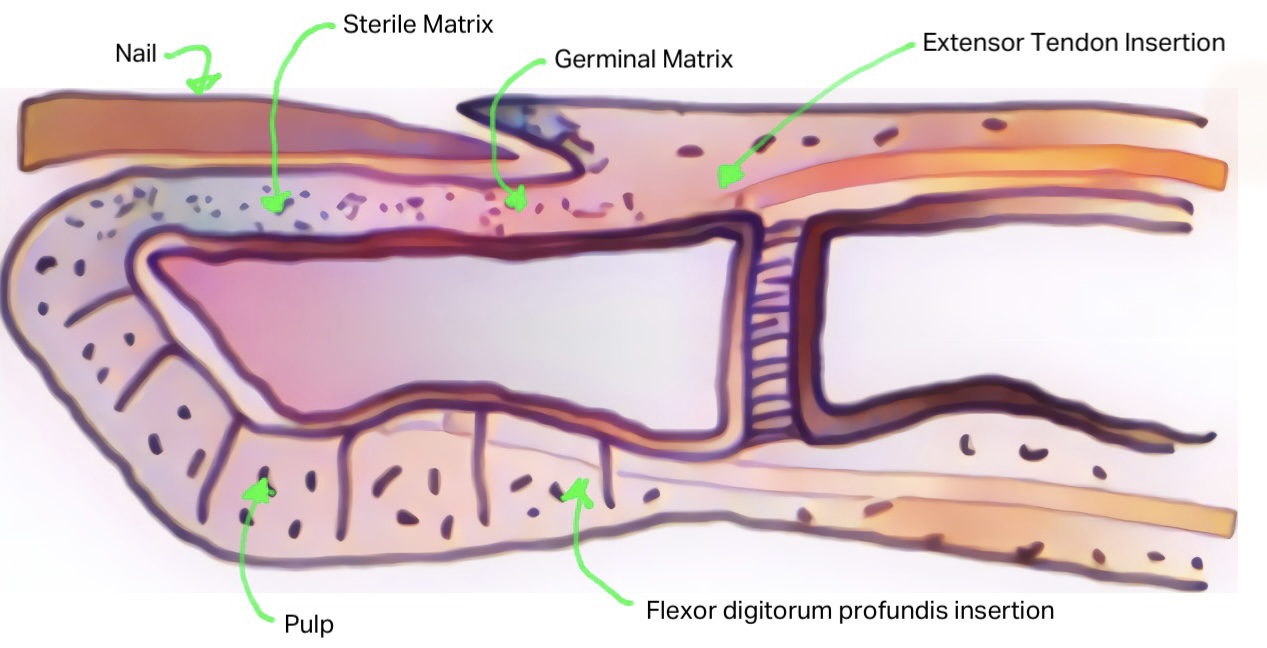
- The proximal and middle phalanges of the hand all possess a head, neck, shaft, and base. In contrast, rather than a head and neck, the distal phalanx starts proximally with a base, then the next part is the shaft, and the most distal portion of bone is the tuft.
- The distal phalanx articulates with the middle phalanx to form the distal interphalangeal joint (DIPJ), which is enveloped by the extensor and flexor tendons along with the volar plate and flanked on the sides by the collateral ligaments.
- And don’t forget this less intuitive tidbit from your anatomy classes: the flexor digitorum profundus (FDP) inserts at the volar metaphysis of the distal phalanx.
- So when we talk about the tuft, we are really talking about the most distal portion of the finger. This is key to recognize because proximal injuries of the distal phalanx have other considerations–like mallet finger formation if the extensor tendon is disrupted, or joint penetration if the fracture is intra-articular.
- All this said, the tuft does happen to be the portion most likely to present to us with an open injury.
Why do we treat this open fracture so differently than we treat other open fractures?
Intuitively, we can all probably agree that all “open fractures” are not the same. There are open fractures where there is a little puncture wound where a long bone may have pierced the skin; then on the other end of the spectrum, there are mangled extremities that are grossly contaminated. So thinking about it this way, it starts to make sense that we shouldn’t necessarily need to treat all of these injuries the same way.
Orthopedic surgeons actually use a grading system for open fractures. The Gustilo-Anderson classification categorizes open injuries into 3 categories, based on wound size, level of contamination, and type of osseous injury.
While we in the ER probably don’t need to memorize or be experts on this system, the upshot of knowing this even exists is that there are certain open fractures that are lower risk than others. This is a well-accepted rubric by which Orthopedic surgeons determine the level of risk associated with an open fracture. This also helps us to understand why orthopedics may make recommendations for one type of open fracture that differ greatly from another.
Truth be told, there aren’t direct studies focused only on open tuft fractures and the decision to washout locally in an ER vs. washout and repair in the OR setting. The closest data I could find was this 2011 study by Capo JT, et al which included all types of open hand fractures, and was retrospective in design. This more recent 2018 study by Bass JT et al was published as an abstract only. It is underpowered and retrospective in design, but also suggests ER washout is likely acceptable management. They emphasize that earlier washout of these injuries is key.
Take-Away:
I believe that uncomplicated distal tuft fractures, excluding severe injuries and proximal distal phalanx fractures (which may have other issues like tendon rupture or joint penetration), can be managed in the ER or Urgent Care setting with proper irrigation, debridement, and primary closure.
How do I splint this thing for the best functional and cosmetic outcome?
A feared outcome with any fracture is non-union (two separate non-fused bone fragments) or malunion (bone fuses, but in a weird way). These can lead to dysfunction, cosmetic deformity, and chronic pain. Fortunately, many non-unions and mal-unions of ther distal phalanx can be asmptomatic for the patient, but splinting is still a good practice to give the bone the best chance of healing properly.
Here are a few things to consider:
In most cases, an external, U-shaped aluminum finger splint is likely good enough. Just be sure to use a shorter one that doesn’t extend over the un-injured proximal interphalangeal joint–otherwise, you may end up with an unnecessarily stiff PIP from the prolonged immobilization.

What if I don’t have access to these? What’s a good substitute in a low resource environment?
Tongue depressors taped on the volar and dorsal aspects of the finger can be a great hack if you can’t access a pre-fabricated finger splint! You can even cut them to a custom length to avoid the PIP/MCP stiffness problem.

Cut the tongue depressor using trauma shears to get the right “custom” length for the patient, immobilizing the DIPJ but leaving the PIPJ mobile to prevent stiffness.

Sandwich the DIPJ and injured tuft with two custom sized tongue depressor ends on the volar and dorsal aspect of the finger. Wrap in coban.

Voila! Custom DIPJ finger splint for the low cost of a tongue depressor and a piece of coban.
Suturing the wound closed and approximating the soft tissue is a splint for the bone.
Don’t forget that just restoring the anatomic alignment of the soft tissues will also bring the pieces of the distal phalanx back in to place, too. This is an acceptable open fracture type for primary closure in the ER or Urgent Care, provided a thorough debridement and washout is performed first.
Replacing the nail is a splint for the bone, too.
While the recently published NINJA trial calls in to question the necessity of replacing a native nail for functional and cosmetic purposes, only a small percentage of these injuries included tuft fractures. In the case of a tuft fracture, the rigidity of a nail can act as a great splint. So consider replanting that native nail if it’s available.
That wraps up Part I. We’ve established that the uncomplicated open tuft fracture can be reasonably treated with an ED washout and splinting.
In Part 2, I’ll address prophylactic antibiotics, follow up care, and tell you about the outcome of this case!
