
This series of posts is meant to expand upon and complement a great article I reviewed that was just published in ALiEM regarding the evaluation and management of extensor tendon injuries. Rather than give redundant information, in these posts, using images and videos, I hope to bring to life some of the specific concepts discussed by Dr. Baylis, Dr. Ting, and Dr. Haythornthewaite.
Evaluation
Explore open injuries thoroughly. This means: good lighting, a bloodless field, adequate exposure (which may mean extending the wound margin) and visualization through a full range of motion.
And here is one more important principle to keep in mind to avoid missing an injury:
Extensor tendon redundancy can mask injury.
There are countless examples. Here are a few specific ones.
Zone IV:
If there is a wound over the dorsum of the proximal phalanx, extension of the proximal interphalangeal joint (PIP) should be examined with the metacarpophalangeal (MCP) joint in extension. If the MCP joint is flexed, the PIP joint may be extended by activation of the lumbrical muscles even if the extensor digitorum tendon is completely divided. Fortunately, this is typically the default position of examination for most practitioners, but can be a pitfall.
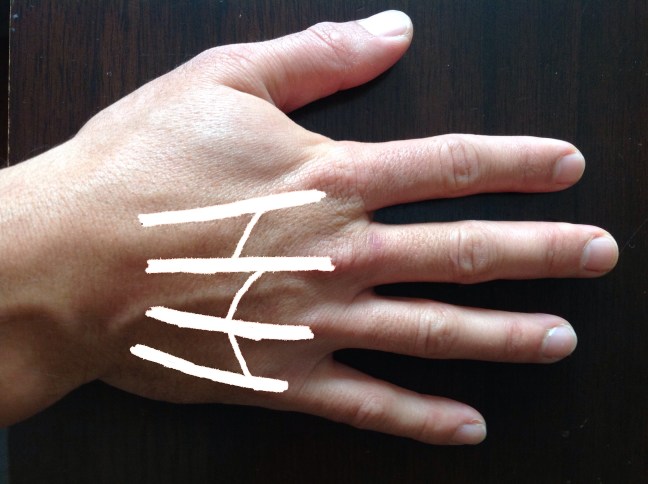
Zone VI:
Over the dorsum of the hand, there are tendinous, ligamentous, and fascial connections between each of the primary finger extensors, called the juncturae tendinum. So, a patient may maintain the ability to extend a digit, albeit weakly, even after a complete tendon laceration. It’s important not just to check extension, but also relative strength in comparison to the contralateral hand!
Digit-Specific
Just to make things harder on you, the index finger and little fingers each have two extensor tendons. Extensor digitorum is common to the 2nd through 5th digit. The index finger ALSO has Extensor indicis proprius, and the pinky finger ALSO has Extensor digitorum minimi. Thus, if one is intact then the patient will still be able to extend the finger even if the other is totally avulsed. Similar redundancy is present in the extension mechanism of the thumb. This redundancy is part of what allows hand surgeons to perform tendon transfers. It is also worth noting that cadaveric studies have shown some variation in the commonly accepted anatomical pattern.

Take Home Points:
- Given the redundancy that is present in the extensor mechanisms, injuries can be subtle.
- Therefore it’s important to test not only active extension but also assess for relative weakness.
- Don’t forget to compare with the best control: the patient’s other hand.
